
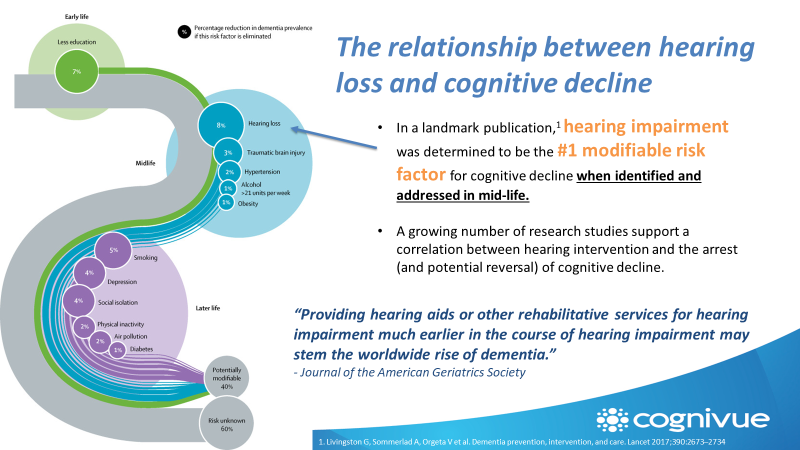
Age-related hearing loss (ARHL) or presbycusis, is the third leading cause of chronic disability in older adults and has been shown to be associated with predisposing cognitive impairment and dementia. Hearing loss has been identified as the number one most modifiable risk factor in preventing dementia and cognitive decline.
Hearing involves hearing two different pathways. The first is peripheral hearing which includes the cochlea, the brainstem, and the auditory nerve. This portion of our hearing is measured in a hearing test which involves the detection of very soft sounds. The other system is our central hearing, also called auditory processing or how our brain puts together sound for the many complex skills needed for hearing such as hearing in noise. Damage to our peripheral hearing affects the clarity and integrity of sound. With a hearing loss when sound reaches the higher areas of the brain for processing the brain has to undergo some reorganization, and will pull from areas which in turn will change the structure of the central systems needed for cognition and hearing. These systems include working memory, recall, ability to focus on sound in noise, and the speed at which we process sound.
Why is hearing loss the most modifiable risk factor in preventing cognitive decline?
Both auditory processes are needed but the question is does weakness in one area, contribute more to cognitive decline? And how do we detect at an earlier stage if there is a weakness or problem in one of these areas? Currently, most diagnosis of hearing loss occurs at age 65 and over. The average loss that is identified at this age is a moderate hearing loss. Evidence indicates that structural changes occur when even a very mild hearing loss is detected. This means that at age 65 structural changes have occurred at least 5 years prior to the identification of hearing loss. Cognitive changes from hearing loss are most likely then present. Most physicians do not screen for cognitive difficulties until the patient is eligible for medicare.
Two things are needed in order to lead vibrant, cognitively sharp, healthy lives.
- The first is to identify hearing loss sooner.
- The second is to determine if hearing loss is causing weaknesses in memory and other cognitive processes.
Until now we did not have a screening test that was clinically proven, and practical for use in audiology clinics. Cognivue is the solution. Cognivue was developed to detect the presence of auditory cognitive dysfunction. The developers have one goal in mind to detect any neurocognitive weakness sooner than is currently being done.
San Francisco Hearing is taking the lead in the San Francisco Bay area to identify hearing loss sooner in order to improve the lives of individuals, their health, wellbeing, cost, family, and society. Join us in our efforts to bring you the very best in care by participating in the cognivue screening the next time you visit our offices.
